Soventus Syrup
1.0 Name of the medicinal product
Ambroxol Hydrochloride, Terbutaline Sulphate, Guaifenesin & Menthol Syrup
2.0 Qualitative and quantitative composition
Each 5 ml Contains:
Ambroxol Hydrochloride IP….20 mg
Terbutaline Sulphate IP……….1.25 mg
Guaifenesin IP……………….50 mg
Menthol IP…………………...0.5 mg
Excipients …... …………………. q. s.
Colour Tartrazine Supra
In a flavoured syrup base
3.0 Dosage form and strength
Syrup
4.0 Clinical particulars
4.1 Therapeutic indication
For the symptomatic relief of bronchospasm in bronchial asthma & chronic bronchitis.
4.2 Posology and method of administration
Adults (12 years & above) 10 ml (2 teaspoonful) 3 times a day.
Children (6-12 years) 5 - 10 ml (1 - 2 teaspoonful) 3 times a day
Paediatric population
Not recommended for children below 6 years of age.
Hepatic & Renal Insufficiency
Caution should be exercised in patients with moderate to severe renal impairment and liver disease.
4.3 Contraindications
- hypersensitivity to any of the components of the formulation.
- patients with pre-existing ischaemic heart disease or those patients with significant risk factors for ischaemic heart disease.
- patients with gastric ulceration.
4.4 Special warnings and precautions for use
In cases of severe renal failure, an accumulation of metabolites formed in the liver must be considered, and a reduction in the maintenance dose of Ambroxol or an increase in the
dose interval must be performed. In patients with a tendency for peptic ulcers, the use of Ambroxol hydrochloride should be carefully considered.
For Terbutaline, caution should be observed in patients with thyrotoxicosis. Cardiovascular effects may be seen with sympathomimetic drugs, including terbutaline.
Guaifenesin should not be used for persistent or chronic cough, such as occurs with asthma, or where cough is accompanied by excessive secretions, unless directed by a physician. Caution should be exercised in the presence of severe renal or severe hepatic impairment. The concomitant use of cough suppressants is not recommended.
Menthol based cough syrups should not be used in consistent and chronic cough with excessive mucin secretions.
4.5 Drugs interactions
The concomitant use of antitussives along with ambroxol may impair the coughing up of the liquefied bronchial mucous and cause a secretory obstruction.
The administration of ambroxol with antibiotics (amoxicillin, cefuroxime, and erythromycin) increases the concentration of antibiotics in bronchopulmonary secretions and sputum.
Terbutaline and non-selective β-blockers should not be administered concurrently. Terbutaline should be used with caution in patients receiving other sympathomimetics. Terbutaline should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants, or within 2 weeks of discontinuation of these agents, since the action of terbutaline on the vascular system may be potentiated.
The concomitant use of menthol cough syrup with warfarin may reduce the therapeutic effects of war farin. Large doses of menthol may affect the felodipine metabolism by inhibiting CYP3A4.
4.6 Use in special populations (such as pregnant women, lactating women, paediatric patients, geriatric patients etc.)
Pregnancy
Since there are no adequate and well-controlled studies of this combination in pregnant women, this medicine should be administered with caution.
Lactation
Terbutaline is secreted into breast milk, but any effect on the infant is unlikely at therapeutic doses. Transient hypoglycaemia has been reported in newborn preterm infants after maternal β-2 agonist treatment. Since Guaifenesin is excreted in breast milk in small amounts, decision must be made to continue with the medicine if benefit of drug outweighs the risks of treatment. It is preferable to avoid use of menthol based cough syrups during pregnancy or lactation.
Geriatric Population
They are more sensitive to the effects of terbutaline; hence a lower dose may be required.
4.7 Effects on ability to drive and use machines
Patients should be cautioned against engaging in activities requiring complete mental alertness, and motor coordination such as operating machinery until their response to Soventus syrup is known.
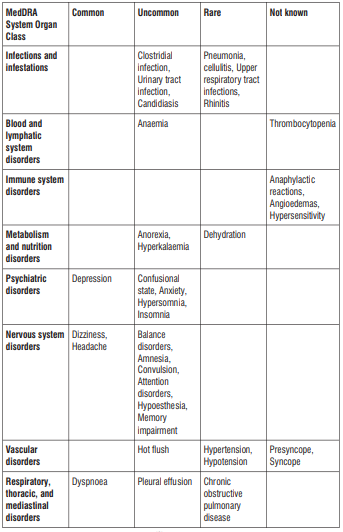
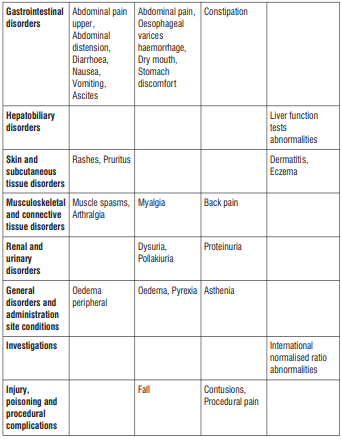
4.8 Undesirable Effects
The most common adverse reactions with Ambroxol are nausea, oral and pharyngeal hypoesthesia, dyspepsia, dry mouth, abdominal pain and allergic reactions such as skin rash or urticaria can also occur.
Tremor and headache are the most common adverse events observed with Terbutaline administration. Tachycardia, palpitations, muscle spasms and hypokalaemia are few other common adverse reactions observed.
Guaifenesin has occasionally been reported to cause gastro-intestinal discomfort, nausea and vomiting, particularly in very high doses. Allergic reactions, angioedema, anaphylactic reactions, dyspnoea (reported in association with other symptoms of hypersensitivity), nausea, vomiting, abdominal discomfort, rash and urticaria may also occur.
Possible side effects from the use of high doses of Menthol are allergic reactions, facial swelling, throat disorder, nausea, vomiting, vertigo, ataxia, drowsiness, exhaustion and stomach pain.
Reporting of suspected adverse reactions
Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit / risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via email to:medico@zuventus.com
Website : http://www.zuventus.co.in/safety.aspx
By reporting side effects, you can help provide more information on the safety of this medicine.
4.9 Overdose
Ambroxol: Symptoms largely correspond with the known adverse effects in case of unintentional overdosing and/or medication errors. Symptomatic treatment is recommended if manifestations of poisoning do occur.
Possible symptoms and signs of Terbutaline overdose is headache, anxiety, tremor, nausea, tonic cramp, palpitations, tachycardia, arrhythmia. A fall in blood pressure sometimes occurs. Hypokalaemia, hyperglycaemia and lactic acidosis may also occur in case of drug overdose. Dose can be reduced in mild and moderate cases whereas gastric lavage or administration of activated charcoal can be followed in severe cases.
The effects of acute toxicity from Guaifenesin may include gastrointestinal discomfort, nausea and drowsiness. The drug is, however, rapidly metabolised and excreted in the urine.
Patients should be kept under observation and treated symptomatically.
Menthol is considered to be safe, and cases of menthol overdose are extremely rare. However, when consumed in large quantities in short span of time may cause heartburn, diarrhoea, dizziness, muscle weakness, mouth sores, skin lesions etc. Treatment should consist of gastric lavage and aspiration.
5.0 Pharmacological properties
5.1 Pharmacodynamic properties
Ambroxol is a metabolic product of bromhexine and possesses mucokinetic (improvement in mucus transport) and secretolytic (liquifies secretions) properties. It promotes the removal of tenacious secretions in the respiratory tract and reduces mucostasis (arresting the secretion of mucus). The breakdown of acid mucopolysaccharide fibers makes the sputum thinner and less viscous and therefore more easily removed by coughing. Although sputum volume eventually decreases, its viscosity remains low for as long as treatment is maintained.
Terbutaline sulphate is an ethanolamine derivative with bronchodilating and tocolytic properties. It selectively binds to and activates β-2 -adrenergic receptors, leading to intracellular adenyl cyclase activation via a trimeric G protein and subsequent increase in cyclic cAMP production. Increased cAMP levels result in relaxation of bronchial and vascular smooth muscle mediated through the activation of protein kinase A (PKA), which phosphorylates proteins in control of muscle tone. cAMP also inhibits release of intracellular calcium ion, reduces calcium entry into cells and induces the sequestration of intracellular calcium. This helps in the relaxation of airway muscles. Terbutaline sulfate also increases mucociliary clearance and reduces release of inflammatory cell mediators.
Guaifenesin is a glyceryl guaiacolate with expectorant effects. It increases respiratory tract mucus secretions, acts as an irritant to gastric vagal receptors and recruits efferent parasympathetic reflexes that cause glandular exocytosis of a less viscous mucus mixture. This provokes cough which facilitates in flushing out tenacious, congealed mucopurulent material from obstructed small airways and lead to a temporary improvement in dyspnea or breathing. This agent reduces the viscosity of mucus secretion by reducing adhesiveness and surface tension as well as increasing hydration of mucus. Guaifenesin increases the efficiency of the mucociliary mechanism which is important in removing accumulated secretions from the upper and lower respiratory tract.
Guaifenesin is a glyceryl guaiacolate with expectorant effects. It increases respiratory tract mucus secretions, acts as an irritant to gastric vagal receptors and recruits efferent parasympathetic reflexes that cause glandular exocytosis of a less viscous mucus mixture. This provokes cough which facilitates in flushing out tenacious, congealed mucopurulent material from obstructed small airways and lead to a temporary improvement in dyspnea or breathing. This agent reduces the viscosity of mucus secretion by reducing adhesiveness and surface tension as well as increasing hydration of mucus. Guaifenesin increases the efficiency of the mucociliary mechanism which is important in removing accumulated secretions from the upper and lower respiratory tract.
5.2 Pharmacokinetic properties
| Parametres | Ambroxol Hydrochloride | Terbutaline sulphate | Guaifenesin | Menthol |
| Tmax | 1.4 ± 0.7 h | 3 h | 15 mins | 3.0 ± 1.2 h |
| Cmax | 29.9·10-6 ± 8.3·10-6 g/l | 20.4 ng/mL | 1.4 ug/ml | 1196 ± 324 ng/ml |
| AUC | 217 ± 54 ng·h/l | 10.7 ng·h/l | 3567.09 ng·h/ml | 3272±543 ng·h/ml |
| Elimination t1/2 | α half-life of 1.3h β half-life of 8.8h | 16 – 20 h | 1 hour | 3.5 ± 0.9 h |
| Metabolism | CYP3A4 is the predominant isoform For ambroxol metabolism. The drug is primarily metabolized in the liver by glucuronidation and partly splitting the dibromo- anthranilic acid (approximately 10% of the dose) along with some other minor metabolites. | It is partially metabolized in the liver to inactive compounds. The main metabolite after oral dosing is the sulphate conjugate. Besides, glucoronide conjugate can also be found in the urine. | Guaifenesin undergo both oxidation and demethylation. | Menthol is metabolized by conjugation with glucuronic acid. Alcohol and hydroxy acid derivatives is produced by cytochrome P450-mediated oxidation. |
| Excretion | During the 3 days of oral administration, 6% of dose remains in free form while approximately 26% of the dose is found in conjugated form in urine. Excretion primarily occurs via the kidneys. | About 90% of the drug is excreted in the urine at 96 hours, with about 60% of this being unchanged drug. Rate of clearance is 311 +/- 112 mL/min. | It is rapidly hydrolyzed (60%within seven hours) and then excreted in the urine, with β-(2- methoxyphenoxy)- lactic acid as its major urinary metabolite. The drug was not detectable in the blood after approximately 8h. | Menthol is excreted in the urine and bile as a glucuronide. |
5.3 Preclinical safety data
Not Available
6.0 NONCLINICAL PROPERTIES
6.1 Animal Toxicology or Pharmacology
No known animal toxicology data.
7.0 DESCRIPTION
Soventus Syrup is a combination of Terbutaline sulphate, Ambroxol hydrochloride and Guaiphenesin. Terbutaline sulphate is a beta-adrenergic agonist bronchodilator available as syrup for oral administration.
Terbutaline sulphate is ±-alpha-[(tert-butylamino) methyl]-3,5-dihydroxybenzyl alcohol sulphate (2:1) (salt).
The empirical formula is (C12H19NO3)2H2SO4 and the structural formula is

Guaiphenesin, a member of methoxybenzenes is an expectorant. The physiologic effect of guaifenesin is by means of decreased respiratory secretion viscosity, and increased respiratory secretions.

Chemical Name: 3-(2-methoxyphenoxy)propane-1,2-diol
Molecular formula: C10H14O4
Molecular Weight: 198.22 g/mol
Ambroxol hydrochloride is an aromatic amine. A metabolite of Bromhexine that stimulates mucociliary action and clears the air passages in the respiratory tract. It is usually administered as the hydrochloride.
Chemical Name: 4-[(2-amino-3,5-dibromophenyl)methylamino]cyclohexan-1-ol;hydrochloride Molecular Formula: C13H19Br2ClN2O Molecular Weight: 414.56 g/mol

8.0 Pharmaceutical particulars
8.1 List of excipients
Disodium Edetate, Sodium Benzoate, Sucralose, Glycerol, Propylene Glycol, Liquid Sorbitol (Non Crystallising), Hydroxyethyl Cellulose, Potassium Sorbate, Colour Tartrazine Supra Soluble , Flavour Ginger RS- 2, Flavour Honey RS 80008, Flavour Lemon RS , Sodium Citrate, Citric Acid Monohydrate.
8.2 Incompatibilities
Not Applicable
8.3 Shelf life
24 MONTHS
8.4 Special precautions for storage
Protect from light.
8.5 Nature and contents of container
1x100ml, PET Bottle
8.6 Special precautions for disposal and other handling
No special requirements for disposal.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
9.0 Patient Counselling Information
- Take this medicine in the dose and duration as advised by your doctor.
- Check the label for directions before use.
- Measure it with a measuring cup and take it by mouth. Shake well before use.
- Soventus Syrup may be taken with or without food, but it is better to take it at a fixed time.
- It may cause dizziness and sleepiness. Do not drive or do anything that requires mental focus until you know how it affects you.
- If you are diabetic, monitor your blood glucose regularly while taking this medicine.
- Inform your doctor if you have a history of thyroid or heart disease.
- Stop taking Soventus Syrup and inform your doctor if your cough persists for more than 1 week, tends to recur, or is accompanied by a fever, rash or persistent headache.
12.0 Date of revision of the text
18th Oct. 2023
About leaflet
Read all of this leaflet carefully before you start taking this medicine because it contains important information for you.
- Keep this leaflet. You may need to read it again.
- If you have any further questions, ask your doctor or pharmacist.
- This medicine has been prescribed for you only. Do not pass it on to others. It may harm them, even if their signs of illness are the same as yours.
- If you get any side effects, talk to your doctor or pharmacist. This includes any possible side effects not listed in this leaflet.
What is in this leaflet:
1. What Soventus® Syrup is and what it is used for
2. What you need to know before you take Soventus® Syrup
3. How to take Soventus® Syrup
4. Possible side effects
5. How to store Soventus® Syrup
6. Contents of the pack and other Information
1. What is Soventus® Syrup and what it is used for
Soventus® Syrup is the combination of Ambroxol Hydrochloride, Terbutaline Sulphate, Guaifenesin & Menthol Syrup.
These active ingredients belong to a group of medicines known as bronchodilators, mucolytic and mucokinetic used to treat asthma, bronchospasm and reversible airways obstruction by widening the airways of the lungs. It is suitable for children or adults who prefer liquid medicines or are unable to use an inhaler device.
Ambroxol hydrochloride widely used as a mucolytic. It increases secretion in the respiratory tract and stimulates ciliary activity. These actions result in improved mucus flow and clearance. Enhancement of fluid secretion and mucociliary clearance facilitates expectoration and reduces cough. Terbutaline sulphate is used as a bronchodilator. It causes bronchodilation, increases mucociliary clearance, suppression of oedema and exerts anti- allergic effects. Guaifenesin is an expectorant that also has some muscle relaxing action. It is used in many cough preparations. This increases the flow of fluids from glands lining the respiratory tract. This results in an increase in volume and decrease in viscosity of bronchial secretions. Menthol is an alcohol produced from mint oils and carries flavouring and local anaesthetic properties. It also has a counterirritant effect on skin and mucous membranes, thereby producing a local analgesic or anaesthetic effect. One of the major effects of menthol when applied to the skin or a mucosal surface is to cause a sensation of coolness; this was attributed to stimulation of thermos-receptors present on the sensory nerves.
2. What you need to know before you take Soventus® Syrup
Do not take Soventus® Syrup if you:
- Hypersensitivity to any of the components of the formulation.
- Pre-existing ischaemic heart disease or those patients with significant risk factors for ischaemic heart disease.
- Gastric ulceration.
Warnings and precautions
In cases of severe renal failure, an accumulation of metabolites formed in the liver must be considered, and a reduction in the maintenance dose of Ambroxol or an increase in the dose interval must be performed. In patients with a tendency for peptic ulcers, the use of Ambroxol hydrochloride should be carefully considered.
For Terbutaline, caution should be observed in patients with thyrotoxicosis. Cardiovascular effects may be seen with sympathomimetic drugs, including terbutaline.
Guaifenesin should not be used for persistent or chronic cough, such as occurs with asthma, or where cough is accompanied by excessive secretions, unless directed by a physician. Caution should be exercised in the presence of severe renal or severe hepatic impairment. The concomitant use of cough suppressants is not recommended.
Menthol should not be used in consistent and chronic cough with excessive mucin secretions.
Other medicines and Soventus® Syrup
The concomitant use of antitussives along with ambroxol may impair the coughing up of the liquefied bronchial mucous and cause a secretory obstruction.The administration of ambroxol with antibiotics (amoxicillin, cefuroxime, and erythromycin) increases the concentration of antibiotics in bronchopulmonary secretions and sputum.
Terbutaline and non-selective β-blockers should not be administered concurrently. Terbutaline should be used with caution in patients receiving other sympathomimetics.
Terbutaline should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants, or within 2 weeks of discontinuation of these agents, since the action of terbutaline on the vascular system may be potentiated.
The concomitant use of menthol cough syrup with warfarin may reduce the therapeutic effects of warfarin. Large doses of menthol may affect the felodipine metabolism by inhibiting CYP3A4.
Soventus® Syrup with food and drink
Fasting bioavailability after oral doses is reported to be about 14 to 15% and is reduced by food.
Use in Special Population:
Pregnancy
Since there are no adequate and well-controlled studies of this combination in pregnant women, this medicine should be administered with caution.
Lactation
Terbutaline is secreted into breast milk, but any effect on the infant is unlikely at therapeutic doses. Transient hypoglycaemia has been reported in newborn preterm infants after maternal β-2 agonist treatment. Since Guaifenesin is excreted in breast milk in small amounts, decision must be made to continue with the medicine if benefit of drug outweighs the risks of treatment. It is preferable to avoid use of menthol based cough syrups during pregnancy or lactation.
Geriatric Population
They are more sensitive to the effects of terbutaline; hence a lower dose may be required.
Pediatric population
Not recommended for children below 6 years of age.
Hepatic & Renal Insufficiency
Caution should be exercised in patients with moderate to severe renal impairment and liver disease.
Effects on ability to drive and use machine
Patients should be cautioned against engaging in activities requiring complete mental alertness, and motor coordination such as operating machinery until their response to Soventus syrup is known.
3. How to take Soventus syrup
Always take Soventus syrup exactly as your doctor has told you. You should check with your doctor or pharmacist if you are not sure.
Taking this medicine
- Take this medicine by mouth.
- If you feel that this medicine is too weak or too strong, do not change the dose yourself, but ask your doctor.
How much to take
Adults (12 years & above): 10 ml (2 teaspoonful) 3 times a day.
Children (6-12 years): 5 - 10 (1 - 2 teaspoonful) 3 times a day.
If you take more Soventus syrup than you should
If you take more Soventus syrup than you should, tell a doctor or go to a hospital casualty department straight away. Take the medicine pack with you. This is so the doctor knows what you have taken.
If you forget to take Soventus syrup
If you forget a dose, do not worry. Just wait until the next dose is due. Do not take a double dose to make up for a forgotten dose.
4. Possible Side Effects
The most common adverse reactions with Ambroxol are nausea, oral and pharyngeal hypoesthesia, dyspepsia, dry mouth, abdominal pain and allergic reactions such as skin rash or urticaria can also occur.
Tremor and headache are the most common adverse events observed with Terbutaline administration. Tachycardia, palpitations, muscle spasms and hypokalaemia are few other common adverse reactions observed.
Guaifenesin has occasionally been reported to cause gastro-intestinal discomfort, nausea and vomiting, particularly in very high doses. Allergic reactions, angioedema, anaphylactic reactions, dyspnoea (reported in association with other symptoms of hypersensitivity), nausea, vomiting, abdominal discomfort, rash and urticaria may also occur.
Possible side effects from the use of high doses of Menthol are allergic reactions, facial swelling, throat disorder, nausea, vomiting, vertigo, ataxia, drowsiness, exhaustion and stomach pain.
Reporting of side effects
If you get any side effects, talk to your doctor. This includes any possible side effects not listed in this leaflet. You can also report side effects directly: Website: www.zuventus.co.in and click the tab “Safety Reporting” located on the top of the home page.
By reporting side effects, you can help provide more information on the safety of this medicine.
5. How to store Soventus Syrup
- Store below 250C, protected from light & moisture.
- Do not throw away any medicines via wastewater or household waste. Ask your pharmacist how to throw away medicines you no longer use. These measures will help protect the environment.
- Keep away from the reach of children. Do not freeze.
6. Contents of the pack and other information
What Soventus Syrup contains
Each 5 ml Contains:
Ambroxol Hydrochloride IP 20 mg
Terbutaline Sulphate IP 1.25 mg
Guaifenesin IP 50 mg
Menthol IP 0.5 mg
Excipients q. s.
Colour Tartrazine Supra
In a flavoured syrup base
1x100ml, PET Bottle
Marketing Authorisation Holder
Zuventus Healthcare Limited
Zuventus House, Plot Y2, CTS No.: 358/A2,
Near Nahur Railway Station,
Nahur (W), Mumbai, 400078 Maharashtra, India.
This leaflet was last revised in 10/2023.